When everything is not about Perimenopause
Not every symptom in your 40s is due to perimenopause and sometimes that assumption delays real answers
Before we begin, I want to acknowledge it is a huge positive step forward for women’s health that perimenopause has become a topic of conversation. Is there still a long way to go when it comes to understanding the nuances? Yes. But at least we have a dialogue.
At the same time, I feel like we’re entering a phase where all symptoms women are experiencing between the ages of 40 and 50 are labelled as perimenopause. Are they sometimes? Yes of course. Is it always? Absolutely not.
For those of you who are just joining me on my blog journey, I use this space to bring real-life situations to light. Today we’re talking about something called a caesarean scar defect (CSD), a condition that many people haven’t heard of, despite the growing number of research papers in the literature.
In its simplest terms it is a pouch that can form at the site of a caesarean section scar.
Why This Conversation Matters
Everyone deserves the ability to make informed choices for their medical care.
It’s now widely accepted that historically most medical research has been conducted on men and that women are often excluded due to their complex physiology. The consequence is that it has taken far too long for women’s health issues to come to the forefront.
A widely recognised example is heart disease: for decades, heart attack symptoms were defined primarily using male presentation patterns, leading to women’s symptoms being overlooked or misdiagnosed.
So, when it comes to gynaecology, we also need to ask, where are the gaps?
How quickly are specialists applying the latest research in practice?
What does this mean for women seeking care today, for symptoms that greatly impact their quality of life?
And perhaps most importantly:
Are women agreeing to treatments that aren’t their preference simply because they weren’t shown all available options?
Why I Care So Deeply About Informed Choice
A large part of the reason I became a naturopath was to support people to make informed decisions about their health care. Choose the path that feels right for you, but everyone deserve access to the information that allows this decision to be informed.
When my youngest son was diagnosed with Eosinophilic Oesophagitis (EoE), we were fortunate to be referred to the RPA Allergy Unit in Sydney. There, we were given the option of treating his condition through an elimination diet. At his last endoscopy, he was still in remission. Why? Because we addressed the root cause and for him, that was the right approach.
So, if you’re still with me, keep reading. What follows is another example from women’s health where symptoms can easily be passed off as ‘just hormones’ or perimenopause. But with the right investigation and informed care, a root-cause approach can apply here too.
Recently, I found myself in this exact position. I did what I always do: I went digging into the research. What I discovered surprised me. I learnt about a relatively newly recognised complication of caesarean sections. When I asked people in my own circle about this, none of them had heard of it either. And yet, how many people do you know who’ve had a caesarean?
What Is a Caesarean Scar Defect (CSD)?
The official definition reads as follows:
A caesarean scar defect (sometimes called a uterine niche or isthmocele) is a small indentation or pouch that can form in the muscle wall of the uterus at the site of a previous caesarean section scar (Murji et al., 2022).
You can think of it as a structural weakness or thinning in the uterus around the scar. Just as a balloon stretches when you blow it up, the thickness of the scar at this point can also vary and become quite thin.
Although caesarean scar defects are only newly recognised, they are not new. As far back as 1959, Poidevin described a depression in the uterus at the site of a caesarean incision (Donnez, 2023). Over the decades that followed, this same finding appeared in the literature under many different names. What has changed is not the condition itself, but our recognition of its clinical relevance. Why has this taken over 60 years…
Studies show these niches can be seen in a significant number of women after a caesarean birth. The size of a caesarean scar defect can influence whether symptoms occur and how severe they are (Wang et al 2009). Although not everyone experiences symptoms, when they occur, they can include (Tsuji, et al., 2023):
Abnormal uterine bleeding
Spotting
Pelvic pain
Painful periods
Dyspareunia
Fertility challenges
Why Do They Develop
There are many associated risk factors for developing this condition (Ducu, et al., 2025; Tsuji, et al., 2023):
Multiple Caesarean deliveries (CD) (rates increase with each subsequent caesarean birth)
Active labour and cervical dilation
Surgical technique used to close the opening in the uterus
Level of uterine incision
Impaired wound healing particularly during the inflammatory phase
Uterine position
Gestational diabetes (only a limited number of studies)
Infections after caesarean deliveries
When Symptoms Look Like Hormones… But Aren’t
Many symptoms of CSD overlap with other conditions, particularly hormonal ones. The table below provides a brief snapshot; key references are at the end of the article.
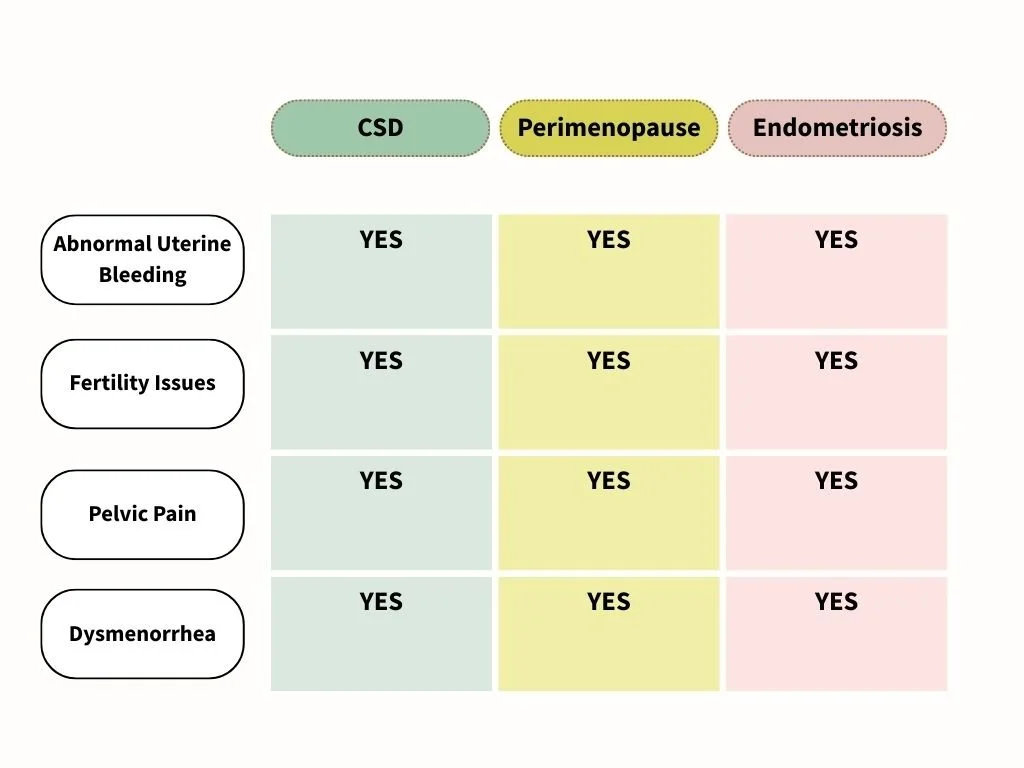
CSD: Caesarean Scar Defect.
Dysmenorrhea is the medical term for painful menstruation, or menstrual cramps, often causing severe pelvic pain, cramps, and nausea during periods.
Menorrhagia is defined as abnormally heavy or prolonged menstrual bleeding (typically lasting over 7 days or soaking through pads/tampons hourly). It is commonly caused by hormonal imbalances, uterine fibroids, polyps, or bleeding disorders.
Let’s just look at one of these shared symptoms; abnormal uterine bleeding (AUB). So what is it?
Clinically, abnormal uterine bleeding is defined as menstrual bleeding that differs from what is considered typical in volume, duration, frequency, or regularity. In simple terms, that might look like (Middelkoop, et al., 2023; Munro, et al., 2019):
Bleeding between periods
Heavy menstrual bleeding
Prolonged postmenstrual spotting
Bleeding that lasts much longer than expected
And this is where things get important. AUB is commonly associated with perimenopause, which makes sense as hormone fluctuations during this transitional phase can absolutely change bleeding patterns. But AUB is also one of the hallmark symptoms reported in women with caesarean scar defects (CSD).
Meaning: the same symptom can stem from completely different root causes.
Why This Matters Clinically
Abnormal uterine bleeding isn’t just inconvenient. Research suggests it affects up to one-third of reproductive-aged women, impacting on physical, mental and social health (Jain et al., 2022). For some women, treatments offered for AUB are broad rather than targeted, and a significant proportion ultimately undergo hysterectomy to resolve symptoms (Jain et al., 2022).
AUB is not a diagnosis. It’s a signal. And signals deserve investigation especially when they could be pointing to different underlying causes that require completely different management approaches.
Treatment Options
Here are some of the approaches currently offered to women to both manage symptoms and/or repair a CSD (Dominguez et al., 2023; Iannone):
Surgical repair
Oral contraceptives
Intrauterine devices
Studies report high success rates for symptom improvement following surgical correction. For example, laparoscopic repair has been associated with postoperative asymptomatic rates ranging from 64% to 100% (Domínguez et al., 2023).
Because a caesarean scar defect is a structural issue, it is important to clearly define the role of naturopathic care. For some women, symptoms are driven primarily by the physical defect itself; in these cases, naturopathic care does not replace the need for surgical assessment or repair.
That said, naturopathic care may still play a supportive role. Interventions can be directed toward symptom management, including heavy or prolonged bleeding, optimisation of iron status, reduction of inflammation, and support of hormonal and tissue health, both while women are considering management options and, where appropriate, before or after surgical intervention.
At present, there is limited published research specifically examining naturopathic or herbal interventions for caesarean scar defects. However, emerging interest in this area is reflected in the recent publication of a protocol for a systematic review and meta-analysis investigating Chinese herbal medicine for the management of caesarean scar defects, suggesting that research in this field is beginning to develop (Deng et al., 2022).
The Importance of the Menstrual Cycle
Spiritual
Not all women feel deeply connected to their menstrual cycle and that’s okay. At the same time, there is a strong revival in this space. Many women already feel this connection, and many more are beginning to explore it.
For those who feel drawn to this perspective, the menstrual cycle is not just a biological process, but a source of insight, creativity, and self-understanding. If you’re interested in exploring this work further, I encourage you to visit Red School, which offers thoughtful resources supporting women to live with empowered knowledge of their bodies and how this flows into health, creativity, leadership, and spiritual life.
As Rose (2022) beautifully states:
‘The reproductive system is part of the entire body, part of Spirit, and part of our whole.’
Health
From a clinical perspective, the menstrual cycle is one of the clearest indicators of a woman’s health.
Changes in bleeding, pain, cycle length, timing, or regularity are not random. They can be early signals that something in the body is out of balance or under strain and your body’s way of communicates that something needs support or investigation.
The reproductive system does not operate in isolation. It is closely linked with hormonal regulation, metabolism, immune function, nervous system health, and emotional wellbeing.
Understanding your cycle is also an act of autonomy
Supporting reproductive autonomy means supporting a woman’s right to understand her body, weigh her options, and choose the path that feels right for her. In naturopathic care, our role is not to decide for women, but to provide the knowledge, clarity, and support needed for informed decision-making (Thakar & Gandhi; 2024)
When women understand their cycles, they are better equipped to advocate for themselves, ask the right questions, and participate actively in their own care.
A Closing Thought
What do we know for sure?
Caesarean scar defects are a recognised complication of caesarean delivery.
Their symptoms often overlap with other gynaecological conditions, which can delay recognition and appropriate care.
Staying current with research and raising awareness helps ensure women are given accurate information and access to the full range of treatment options.
Women should never feel pressured to accept care that isn’t aligned with their preferences.
Because understanding your body should never be optional.
Notes
During perimenopause and menopause, hormonal shifts particularly the decline in oestrogen can influence musculoskeletal health. Many women notice increased joint pain, stiffness, muscle loss, and changes in bone density, which can affect both physical comfort and overall quality of life (Chaudhary et al.,2025). I am highlighting this as pelvic pain can fall into this category for some women as per Table in text.
References
Chaudhary, P., Rajpurohit, P., & Zeeshan, M. (2025). Physiotherapy Approaches to Managing Musculoskeletal Pain During Menopause and Perimenopause: A Systemic Review. International Journal for Multidisciplinary Research, 7(2), 2582-2160.
Deng, J., Li, S., Peng, Y., Chen, Z., Wang, C., Fan, Z., ... & Jiang, Y. (2020). Chinese herbal medicine for previous cesarean scar defect: a protocol for systematic review and meta-analysis. Medicine, 99(50), e23630.
Dominguez, J. A., Pacheco, L. A., Moratalla, E., Carugno, J. A., Carrera, M., Perez‐Milan, F., ... & Alcázar, J. L. (2023). Diagnosis and management of isthmocele (Cesarean scar defect): a SWOT analysis. Ultrasound in Obstetrics & Gynecology, 62(3), 336-344.
Donnez, O. (2023). Cesarean scar disorder: management and repair. Best Practice & Research Clinical Obstetrics & Gynaecology, 90, 102398.
Ducu, I., Salmen, B. M., Iordache, A. M., Durdu, C. E., & Bohiltea, R. E. (2025). Ranking of risk factors leading to uterine scar defect—systematic online review. Journal of Clinical Medicine, 14(13), 4551.
Iannone, P., Nencini, G., Bonaccorsi, G., Martinello, R., Pontrelli, G., Scioscia, M., ... & Scutiero, G. (2019). Isthmocele: from risk factors to management. Revista Brasileira de Ginecologia e Obstetrícia/RBGO Gynecology and Obstetrics, 41(01), 044-052.
Jain, V., Chodankar, R. R., Maybin, J. A., & Critchley, H. O. (2022). Uterine bleeding: how understanding endometrial physiology underpins menstrual health. Nature reviews endocrinology, 18(5), 290-308.
Middelkoop, M. A., Don, E. E., Hehenkamp, W. J., Polman, N. J., Griffioen, A. W., & Huirne, J. A. (2023). Angiogenesis in abnormal uterine bleeding: a narrative review. Human reproduction update, 29(4), 457-485.
Munro, M. G., Critchley, H. O., Fraser, I. S., FIGO Menstrual Disorders Committee, Haththotuwa, R., Kriplani, A., ... & Warner, P. (2018). The two FIGO systems for normal and abnormal uterine bleeding symptoms and classification of causes of abnormal uterine bleeding in the reproductive years: 2018 revisions. International Journal of Gynecology & Obstetrics, 143(3), 393-408.
Murji, A., Sanders, A. P., Monteiro, I., Haiderbhai, S., Matelski, J., Walsh, C., ... & of Gynecology, T. I. F. (2022). Cesarean scar defects and abnormal uterine bleeding: a systematic review and meta-analysis. Fertility and sterility, 118(4), 758-766.
Nezhat, C., Zaghi, B., Baek, K., Nezhat, A., Nezhat, F., Lindheim, S., & Nezhat, C. (2023). Outcomes of laparoscopic cesarean scar defect repair: retrospective and observational study. Journal of Clinical Medicine, 12(11), 3720.
Thakar, R., & Gandhi, M. (2024). Reproductive autonomy: women’s health and rights. Authorea Preprints.
Tower, A. M., & Frishman, G. N. (2013). Cesarean scar defects: an underrecognized cause of abnormal uterine bleeding and other gynecologic complications. Journal of minimally invasive gynecology, 20(5), 562-572.
Tsuji, S., Nobuta, Y., Hanada, T., Takebayashi, A., Inatomi, A., Takahashi, A., ... & Murakami, T. (2023). Prevalence, definition, and etiology of cesarean scar defect and treatment of cesarean scar disorder: a narrative review. Reproductive medicine and biology, 22(1), e12532.
Wang, C. B., Chiu, W. W. C., Lee, C. Y., Sun, Y. L., Lin, Y. H., & Tseng, C. J. (2009). Cesarean scar defect: correlation between Cesarean section number, defect size, clinical symptoms and uterine position. Ultrasound in Obstetrics and Gynecology, 34(1), 85-89.